Hello, and welcome back! Firstly, I must apologise for such a prolonged absence. I can’t quite believe it has been so long since my last blog post but I seem to have managed to keep myself very busy with a number of things. Regardless, we shall crack on with having a look through the different critical care and anaesthesia literature out there that is waiting to be devoured. Given that I have currently just started a block of neuro-critical care, I felt it was a good time to have a look at some of the big studies in this area, especially as there have been a few interesting ones recently. Today I’ve opted to have a look at the RESCUEicp study which came out in September last year. The full text is available at the link below, and I’d definitely recommend having a look at it as well as just reading my rambling thoughts. I’ve also put together a more focused review of the paper here [link] if you want to read a bit more of the details.
The RESCUEicp Study
The RESCUEicp Study
What's it about?
I think it’s fairly well know that traumatic brain injury isn’t a great thing. As well as the obvious focal injuries that can occur (extradurals etc.) the diffuse injury to the brain as a whole causes some significant problems. Whilst in the long term these can seriously affect the functional recovery of the patient, it is also a problem for us intensivists in the short term because of the tendency for oedema to develop in the hours and days following the injury. When we are trying the prevent secondary insults to an already fragile brain, this swelling causes all sorts of problems in achieving this, particularly with elevations in intracranial pressure (ICP) and its impact on reducing the perfusion of the brain tissue. As such, traumatic brain injury protocols now often use a tiered approach to manage this common complication, starting with simple things like minimising venous obstruction and nursing head up, through to hypertonic saline or mannitol therapy. The big challenge is when you have depleted all your medical options and yet are still trying to fit 1500cm3 of brain into the 1300cm3 box that is the skull. The typically surgical response is to ‘get a bigger box’ and thus decompression of the cranial cavity has been employed by taking part of the skull away, thus allowing the swollen brain a bit more breathing room until all that acute badness has settled down.
This makes a decent bit of sense, but is it cracking open the skull actually good for our patients? This was the question that the investigators of the RESCUEicp study wanted to answer. A precedent to this trial was the DECRA study, which trialed taking part of the skull off ‘prophylactically’ to see if this would be better than exhausting all other options first. Unfortunately it wasn’t, and the study showed worse outcomes for those who has early decompressive craniectomies. As such the investigators here wanted to know whether this very invasive procedure is actually ever worth doing and turned their gaze on the remaining use of decompression as a last resort.
What did they do?
The study was a muticentre randomised control trial looking at the best approach to patients who still had elevated ICP after all tier 1 and 2 therapies had been implemented (i.e. pretty much all options exhausted). If ICP remained over 25mmHg for at least an hour, and other inclusion/exclusion criteria were met, then they were randomised to either decompressive craniectomy or maximal medical therapy. Maximal medical therapy in this case almost universally meant a barbituate coma (barbituates weren’t allowed any earlier than this), but with continuation of all tier 1 and 2 therapies in both groups.
The outcome they were looking at was the well recognised Extended Glasgow Outcome Score (GOS-E)[Link], initially at 6 months (primary outcome) and also at 12 and 24 months. This is a well recognised 8-point scale ranging from death through to a good neurological outcome with no disability. There was some degree of subjectivity as to which classes constituted a ‘good outcome’ but the investigators decided to vary common practice and classify ‘Upper Severe Disability’ or better as a ‘good outcome’. Upper severe disability means that the patient is able to be live at home and be left on their own for up to 8 hours, but still has significant care needs. Other outcome measures included looking at the impact on ICP, duration of hospital stay and quality of life outcomes.
What did they find?
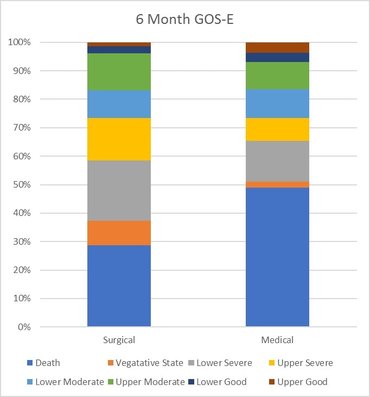
The results were very interesting. The study showed a clear reduction in the number of patients dying (26.9% vs 48.9% at 6 months). Well that’s great then, everyone can get the top of their skulls taken off and things will be ok! I can hear the neurosurgeons powering up their saws from here. However, the other outcomes also paint a very important picture. When looking at the ‘lower quality’ outcomes there is also a notable difference between the groups. At 6 months the number of patients in a vegetative state in the craniectomy group was 8.5% vs 2.1% in the medical group, the number in a lower severe disability group was 21.9% vs 14.4%, and in the upper severe disability group was 15.4% vs 8% (although this could be considered a ‘good outcome’). Although the study wasn’t powered to analyse the statistical difference between the subgroups in this way, it paints a very interesting picture, that is perhaps most easily appreciated in graphical form (see below). In essence, the concern is that the result of the decompressive craniectomy is to save the life of the patient, but they are then left with significant neurological morbidity.
Is it any good?
Well I think this is a good study and certainly trying to answer a very pertinent question. The study has been run in a pragmatic way and I think it probably does reflect clinical practice pretty well. The outcomes they have looked at are probably the most important ones, and despite the statistical challenges, they have described the results well to aid our interpretation. Most notably, there was a pretty high degree of crossover from the medical to the surgical arm (37.2%), but I think this would have primarily diluted the impact of the surgical intervention. You could perhaps talk yourself into the argument that it might be these patients that are the ones with the increased number of poor outcomes, because of a greater time with a raised ICP whilst medical therapy failed, and I wonder if this sub-group could have provided a lot of useful information.
The problem with it is that I think it might raise more questions than it answers. It moves the forum of the debate from a scientific domain about the strengths of the evidence, to an ethical domain, and the question of what is the right thing to do based on these principles. There isn’t a dichotomy of outcome here as there often is in clinical trials, and the impact of neurological morbidity is something that is very difficult to classify (and in my opinion is probably completely unique to each patient). Even if I think about it now, I can’t decide what degree of disability I would be happy to accept for myself to carry on living. I can’t picture what degree of happiness I could find in life just from my imagination, and I can well imagine that I could be grossly overestimating or underestimating it. How we can do this for our patients, whilst they are unconscious, through their distraught family members, and with a fairly urgent time pressure, I have no idea.
Final THoughts
Overall, I think this is a very eye-opening study. It suggests (but by no means demonstrates) that decompressive craniectomy can be life-saving for our patients with worsening ICP when almost all other options have been exhausted. However, it may be that this will result in more patients surviving with worse neurological outcomes. Whether this is therefore the right thing to do is not something that no RCT can ever answer. It provides us a bit more information which we can use to help do what is (hopefully) right for each individual patient, depending on their specific circumstances, beliefs and wishes.
Thanks again for reading, and please leave any comments or thoughts you might have, especially if you think this has impacted your own practice in any way. Hopefully, there will be a much smaller gap until the next blog and I hope to see you back here then.
BW
Tom Heaton
BW
Tom Heaton
Links & References
- Hutchinson P et al. Trial of decompressive craniectomy for traumatic intracranial hypertension (RESCUEicp Trial). 2016. NEJM. 375: 1119-1130. Avaialble at: http://www.nejm.org/doi/full/10.1056/NEJMoa1605215#t=article
- TheBottomLine. RESCUEicp. 2016. A great appraisal of the key points of the paper. Available at: http://www.thebottomline.org.uk/summaries/icm/rescue-icp/
- Cooper D et al. Decompressive craniectomy in diffuse traumatic brain injury (DECRA Trial). NEJM. 2011. 364: 1493-1502. Available at: http://www.nejm.org/doi/full/10.1056/NEJMoa1102077#t=article
Image courtesy of www.freedigitalphotos.net and Stockdevil
 RSS Feed
RSS Feed
