Last week I went along to my 2nd PeriopMan event of the year, attending the annual meeting at the Manchester Conference Center. The day continued the impressive trend that I enjoyed at their anaemia half-day earlier in the year, bringing together some excellent speakers covering a wide range of topics. We were also privileged enough to be invited to attend to run a stand for NWRAG and in this blog I’ve tried to put summarise a few of the highlights of the day.
Getting it Right First Time
Danny Conway (deservedly now a professor) opened the day talking about ‘getting it right the first time in perioperative medicine’ (slightly burdened by the acronym GIRFT). As a slight aside, he opened his talk with a quick teaser about an upcoming perioperative medicine masters course at Manchester Metropolitan University, although there are still a few aspects to be completed. Exciting news for any readers with a strong interest in further education in this area. But back to the main theme, if you haven’t heard of it before, GIRFT is a programme developed across the NHS to try and improve the quality of care, and in particular reducing unwarranted variation. Now variation is not always a bad thing; there needs to be some bespoke response to local problems and needs, and innovation should be actively encouraged. However, it is important to recognise that there can be unwarranted variation that may potentially be negatively impacting on patient outcomes, as well as costs. As an example of the potential impact, the Carter Report 2016 noted that the national variation in costs could be costing the NHS a whopping £5 billion (the potential savings if providers’ cost bases were actually all at the median level).
A lot of the data that GIRFT uses is drawn from data that are already collected; coding, the national hip fracture database, NELA, etc. This is supported by data that individual departments submit (which is quite extensive), and then analysed to look at what variation is occuring. The questions are then around whether this variation is likely to be relevant, and with the results subsequently being published both locally and nationally. A number of these reports have been undertaken already different surgical specialties nationally and are underway in some of the specialties we are most interested in: anaesthesia, perioperative medicine and critical care. As an example of the insights they may provide, the general surgical report shows variation in demand, activity, decision making and outcomes. These report allows comparison of local sites to their ‘peers’ across the country, making benchmarking possible, and potentially driving changing.
I find this use of data exciting, if not without a few slight concerns. Some of the changes that have already been implemented from such reports sounds very interesting, with changes to care structure (e.g. consultant triage) and adjustment of equipment use to impact on costs. My concerns, as were touched on in some of the Q&As at the end, would include problems with gaming the system, and the potential misapplication of findings. However, the approach is described as constructive rather than accusatory, and indeed it seems very valuable to identify areas for potential improvement as well as areas of excellence. There is ongoing work on perioperative medicine, including in the Northwest, with a focus on the 3 strands of daycase surgery, enhanced recovery (major elective), and emergency surgery e.g. laparotomies, neck of femur fractures. It will be interesting to hear more about the results of this process in the near future.
A lot of the data that GIRFT uses is drawn from data that are already collected; coding, the national hip fracture database, NELA, etc. This is supported by data that individual departments submit (which is quite extensive), and then analysed to look at what variation is occuring. The questions are then around whether this variation is likely to be relevant, and with the results subsequently being published both locally and nationally. A number of these reports have been undertaken already different surgical specialties nationally and are underway in some of the specialties we are most interested in: anaesthesia, perioperative medicine and critical care. As an example of the insights they may provide, the general surgical report shows variation in demand, activity, decision making and outcomes. These report allows comparison of local sites to their ‘peers’ across the country, making benchmarking possible, and potentially driving changing.
I find this use of data exciting, if not without a few slight concerns. Some of the changes that have already been implemented from such reports sounds very interesting, with changes to care structure (e.g. consultant triage) and adjustment of equipment use to impact on costs. My concerns, as were touched on in some of the Q&As at the end, would include problems with gaming the system, and the potential misapplication of findings. However, the approach is described as constructive rather than accusatory, and indeed it seems very valuable to identify areas for potential improvement as well as areas of excellence. There is ongoing work on perioperative medicine, including in the Northwest, with a focus on the 3 strands of daycase surgery, enhanced recovery (major elective), and emergency surgery e.g. laparotomies, neck of femur fractures. It will be interesting to hear more about the results of this process in the near future.
Do Children Need Preop Assessment?
Next up was Dr Simon Courtman (@apagbi), a consultant paediatric anaesthetist from Plymouth, talking about whether children need preoperative assessment. As Simon notes, the majority of periop medicine is focused on adults, with children rather being left to it. Simon has been heavily involved in perioperative work, more specifically from the paediatric perspective, and notes that this relative indifference is represented in the national perioperative approach. Children are generally thought to be low risk, almost universally fairly fit and well (although obviously some clear exceptions), and thus the benefits of providing pre-op assessment seem less relevant. A major challenge then becomes money (as it often is) as there are fewer obvious benefits to trusts from providing this service to children. The benefits in adults are widespread and include financial savings, increased satisfaction, and reducing cancellations and DNAs, amongst many others. Simon effectively argued that there is actually a lot more overlap with paediatric practice here than is presumed, and some of the work that has been done at Plymouth supports this. Even from just baseline values, we can see that about 20% of children undergoing procedures have complex medical conditions or are undergoing complex surgery. Work at Plymouth to implement a preoperative assessment service has suggested that about 40% of children had issues identified that may have delayed the list on the day. As well as identifying potential problems that may delay the surgical list on the day, the visit had provided the patients and parents with a wealth of invaluable information, allowed an increased familiarity with the environment, and better coordination of fasting. Anxiety in both parents and children was reduced and parents were invariably happier with attending pre-op assessment, despite the ‘hassle’ that it often involved. It sounds like this importance is being recognised, including with an increased focus in the new curriculum and the GPAS preoperative assessment document which will be interesting to watch. You may also want to check out the Little Journey App as a great example of some innovation in practice in this domain.
The Global Landscape of Airway Management
Prof Ellen O’Sullivan (@ProfEllenO) was next to deliver the keynote speech on ‘The global landscape of airway management’. That Prof O’Sullivan has an interest in airway management is a slight understatement and she brought a wealth of expertise to her talk on airway management. NAP4 remains the landmark study here, despite its increasing age, due to the quality of the study and the value of its findings. Having only ever practised anaesthesia in the post-NAP4 period, it is fascinating to reflect on the impact it has had on clinical practice. I can barely imagine intubating a patient without the presence of waveform capnography, and that would seem to be strongly related to the impact of this study and related work. It is a little concerning to see that the well described problems have not disappeared. Even with the numerical data on this it is probably the individual patient stories carry the greatest weight. Hearing tales of undetected oesophageal intubation leading to anoxic brain injury and death that have occurred in just the past few years is saddening.
This led onto the importance of strategies to manage such problems, and the DAS can't intubtae, can't oxygenate (CICO) algorithm is another piece of work that I can barely imagine a world without. The current guideline (from 2015) was only the 2nd iteration, and yet is such a key piece of work. Despite the importance of the guidance there has been quite a bit of debate about the approach to front of neck access (FONA), with the scalpel vs needle question causing a fair degree of controversy. The use of ‘The Airway App’ seems to be a great project to gain valuable information on such rare events. Incidents of FONA from around the world can be reported through the app, and the details provided on the factors involved analysed to try and glean nuggets of invaluable information. You can read more about the findings in this review in Anaesthesia, with perhaps the most interesting finding being that the scalpel-bougie success rate was the highest.
This led onto the scoop of the day; the first presentation of the new DAS awake tracheal intubation guidelines! The purpose of this again links back to the findings of NAP4. Despite there often being an appropriate indication for awake intubation, this approach to securing the airway was underutilised. Now although traditionally this has been a fibreoptic approach, there has been the description of using a similar approach to facilitate awake intubation using videolaryngoscopy (as we covered in the NWAM blog). Although the complication and failure rates with such an approach are both low (around 1%) it is also a technique that is rarely used by many anaesthetists. Indeed, this was one of the arguments that Dr Andrew Smith has employed to advocate for the videolaryngoscope approach, noting that this is a tool that many anaesthetists are very familiar with. The goal of the new DAS guidance was therefore to bring together a document that could help clinicians have a clear approach that they could use, including support on managing potential challenges. The full document will be fully unveiled at WAMM at the start of November and will certainly be worth keeping an eye out for. Some key learning points that I took away included:
This led onto the importance of strategies to manage such problems, and the DAS can't intubtae, can't oxygenate (CICO) algorithm is another piece of work that I can barely imagine a world without. The current guideline (from 2015) was only the 2nd iteration, and yet is such a key piece of work. Despite the importance of the guidance there has been quite a bit of debate about the approach to front of neck access (FONA), with the scalpel vs needle question causing a fair degree of controversy. The use of ‘The Airway App’ seems to be a great project to gain valuable information on such rare events. Incidents of FONA from around the world can be reported through the app, and the details provided on the factors involved analysed to try and glean nuggets of invaluable information. You can read more about the findings in this review in Anaesthesia, with perhaps the most interesting finding being that the scalpel-bougie success rate was the highest.
This led onto the scoop of the day; the first presentation of the new DAS awake tracheal intubation guidelines! The purpose of this again links back to the findings of NAP4. Despite there often being an appropriate indication for awake intubation, this approach to securing the airway was underutilised. Now although traditionally this has been a fibreoptic approach, there has been the description of using a similar approach to facilitate awake intubation using videolaryngoscopy (as we covered in the NWAM blog). Although the complication and failure rates with such an approach are both low (around 1%) it is also a technique that is rarely used by many anaesthetists. Indeed, this was one of the arguments that Dr Andrew Smith has employed to advocate for the videolaryngoscope approach, noting that this is a tool that many anaesthetists are very familiar with. The goal of the new DAS guidance was therefore to bring together a document that could help clinicians have a clear approach that they could use, including support on managing potential challenges. The full document will be fully unveiled at WAMM at the start of November and will certainly be worth keeping an eye out for. Some key learning points that I took away included:
- Utilising nasal high flow oxygen can provide the well recognised benefits of the technique without actually getting in the way too much.
- Sedation is definitely not a substitute for adequate airway topicalisation.
- It’s difficult to see if there is any difference between a fibre-optic or videolaryngoscope technique.
An excellent keynote speech from @ProfEllenO on airway management. The new DAS awake intubation guidelines sound interesting #periopman19
— Thomas Heaton (@tomheaton88) October 4, 2019
Perioperative Optimisation of Antibiotics
Prof Van De Waele (@criticcaredoc) delivered the final talk of the morning, discussing antibiotics in critical care. Antibiotics and source control are really the few options available to definitively manage sepsis, the rest being purely supportive. However, a significant amount of antibiotic use on critical care remains inappropriate (he quotes a huge 30-60%!). In addition, there are significant challenges posed by the nature of critical illness that influences our use of antibiotics. If we think about the 3 main factors of antibiotic care: micro-organism, pharmacodynamics (PD) and pharmacokinetics (PK), we can see that there are a number of negative effects from the disease process. As a quick example, the microorganism can be unknown, the volume of distribution can be notably increased, and clearance of the drug can actually be increased (in as high as 30-50% of patients), all potentially leading to the patient receiving an inadequate dose of antibiotics. Even without these challenges, we are commonly not paying attention to the concept of loading patients, something that is quite obvious when we stop and think about the pharmacokinetics. Subsequently, plasma levels of antibiotics are often highest at day 5-7, when we actually want them high right from the start or treatment, especially in cases of severe sepsis. The subsequent failure to achieve the minimal inhibitory concentration (MIC) has some significant implications. Being below the MIC unsurprisingly results in impaired bacterial killing, but also a worrying rise in resistance levels. This isn’t relevant to all antibiotics, with peak concentration being more important in some cases e.g. aminoglycosides, but the ‘workhorse’ of antibiotics in healthcare, the beta-lactams, do need this continuously high plasma level. Essentially, you really need to be above the MIC 100% of the time, and probably a good deal higher in patients that are critically ill. This is a good part of the argument behind continuous infusion strategies, with greater control over the length of time that will be spent above MIC. Prof Van De Waele promotes the employment of an approach that considers the PDPK target (e.g. MIC, peak concentration), giving an appropriate loading dose to reach therapeutic labels, and then establishing a maintenance plan. The BLING3 study will hopefully tell use a bit more information about the role of an infusion strategy to manage this problem, although another way we may improve our approach is through the monitoring of drug levels. Whilst this is currently mainly used to assess for toxicity risk, they are increasingly being employed to assess for efficacy, especially in populations like this where the normal PK models (based on healthy volunteers) are less useful.
Breakout Sessions
After an excellent lunch, the afternoon started with a selection of 5 breakout sessions with a broad choice of topics. I picked the sessions on artificial intelligence (AI) and sim wars, which both proved to be a good choice. The session on AI was particularly fascinating, with a real glimpse into the (perhaps not so distant) future. The speakers from Edwards described the use of AI to deeply analyse arterial waveforms to be able to accurately predict patients who were on their way to developing hypotension. Such machine learning provided some impressive AUROC results, and they had done a good job of integrating it into monitoring technology. They discussed how the next step is to move on to effective prescriptive AI, bringing in an efferent limb to the closed-loop system. My personal thoughts are that I think there is probably still a bit of a gulf between the ability to be highly predictive over a specific parameter (e.g. blood pressure) and to then derive an appropriate response. This first component seems very reasonably within the reach of narrow AI, and is something that I truly believe it will be better at than us. However, I think bringing together the complex interactions of multiple, incompletely understood systems, which is the essence of medicine, is beyond the scope of narrow AI, and we might have to await something closer to general AI. Regardless of my ill-informed opinions, this is an exciting area and I am certain we will be seeing more AI helping us deliver better medical care in the near future.
Here are some further interesting links on the topic:
AI for anaesthesia
Machine learning algorithm to predict hypotension
This is also a fascinating podcast on the topic
Here are some further interesting links on the topic:
AI for anaesthesia
Machine learning algorithm to predict hypotension
This is also a fascinating podcast on the topic
THoracic Epidurals
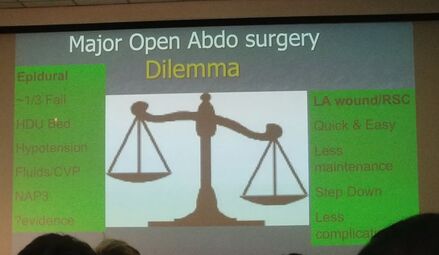
The day closed with a pro-con debate on the role of thoracic epidurals in major open abdominal surgery. Dr Rick Makin (@gasmakin) started by pioneering the con side of the debate. Although he did an excellent job of presenting an approach to the pros and cons of thoracic epidurals, his arguments attacked both their efficacy (a purported strength) whilst reiterating the many challenges that their use entails. One aspect of the problem of epidurals comes from a safety aspect; bleeding, infection (although both rare), and the more frequent requirement for CVS support. They also have a significant technical challenge, being hard to put in and having a tendency to ‘fall out’ on the ward, both contributing to a not insignificant failure rate. He argued that the evidence suggested that the use of appropriate local anaesthesia techniques (rectus sheath catheters being the main example) with some opioid for visceral cover was no worse. When then considering the challenges of employing epidurals (insertion, subsequent care, etc.) they seemed to be the less good option.
Dr Oliver Pratt led the charge for the pro side, focusing his argument along the lines of analgesia and outcome benefits. The evidence base is challenging, but epidurals have been convincing demonstrated as better than opioids (Cochrane 2016). In contrast, much of the work looking at the newer regional stuff has been non-inferiority, retrospective, or simply not comparing like with like. In addition, whilst not completely benign, NAP3 shows a decent safety profile. Certain other side effects, such as delayed return of GI function and respiratory complications, are better with epidurals, and ERAS still recommends their use. A problem then arises with the reducing use of this technique, as it is a skill that it is important to maintain and be proficient at to get the best results. If we move away from performing them regularly, it may become an area that we deskill in. A point of interest was when the question was asked at the end “as an anaesthetist, which would you rather have?”. For major abdominal incisions, the answer does still seem to be an epidural, although the final vote was only a 55 to 45 favour to the pro side (essentially unchanged from the initial vote). I think that that is the way that I would still lean, although it is reassuring to know that there are other decent options for pain relief in our armamatarium, which is never a bad thing.
These were some of the references that they used:
Cochrane: Epidurals vs systemic opioids.
Thoracic epidural anaesthesia.
NAP 3.
Rectus sheath catheters.
Dr Oliver Pratt led the charge for the pro side, focusing his argument along the lines of analgesia and outcome benefits. The evidence base is challenging, but epidurals have been convincing demonstrated as better than opioids (Cochrane 2016). In contrast, much of the work looking at the newer regional stuff has been non-inferiority, retrospective, or simply not comparing like with like. In addition, whilst not completely benign, NAP3 shows a decent safety profile. Certain other side effects, such as delayed return of GI function and respiratory complications, are better with epidurals, and ERAS still recommends their use. A problem then arises with the reducing use of this technique, as it is a skill that it is important to maintain and be proficient at to get the best results. If we move away from performing them regularly, it may become an area that we deskill in. A point of interest was when the question was asked at the end “as an anaesthetist, which would you rather have?”. For major abdominal incisions, the answer does still seem to be an epidural, although the final vote was only a 55 to 45 favour to the pro side (essentially unchanged from the initial vote). I think that that is the way that I would still lean, although it is reassuring to know that there are other decent options for pain relief in our armamatarium, which is never a bad thing.
These were some of the references that they used:
Cochrane: Epidurals vs systemic opioids.
Thoracic epidural anaesthesia.
NAP 3.
Rectus sheath catheters.
Well thank you for reading. I hope the blog piqued your interest on a few topics, and hopefull the links can expand on some of these still further. I had a very enjoyable and educational day and can strongly recommend checking out PeriopMan’s future events.
Tom
Tom
 RSS Feed
RSS Feed
