By Tom Heaton

This week it was my turn to present a paper at our local journal club. After a bit of searching for an exciting paper, I settled on this paper looking at the effect of age on spinal anaesthetic dose requirements. ‘The Effect of Age on the Median Effective Dose (ED50) of Intrathecally Administered Plain Bupivacaine for Motor Block’ was looking at an area of anaesthetic practice that I had been meaning to look into for a while; namely to see what evidence was out there about the factors that impact on the effectiveness of spinals. This interest was piqued by some recent reading around hip fracture management, including the National Hip Fracture Database Sprint Audit, which highlight problems with intraoperative hypotension as well as the rather large range of local anaesthetic doses used. How low can we go with our doses? Is there any point in going low with them? What factors impact on the dose we give? This paper starts having a look at this topic with some interesting results.
What's It About?
Well the paper aims to quantify the changes that age has on the median effective dose needed for effective spinal anaesthesia. As such they split eligible patients into cohorts for different decades of life (20-30, 31-40, etc) and used a technique called up-down sequential allocation to find this median effective dose.
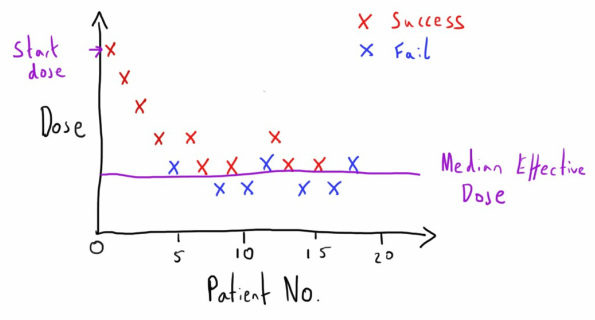
Up-down what? This was my first question when reading this paper having never come across the approach before, so I’ll take a couple of lines and a dodgy drawing to try and explain it. This design uses the outcome of the patient before the current patient to determine what dose you will use. A success-fail binary outcome is predetermined (in this case the degree of motor blockade) and a predetermined starting dose is given to the first patient (in this case 7.5 mg of 0.75% plain bupivicaine). If the result is a success then the next patient gets a dose that has been reduced by a predetermined aliquot (0.75mg) and they see if this is a success or a fail. When a patient has a ‘fail’ outcome, the next patient gets their dose increased by the predetermined aliquot. This continues with the dose going up and down depending on the success or failure of the dose with the preceding patient. The result is an oscillation around the median effective dose that we are interested in. If there are 6 or more oscillations then we can be reasonably confident with the median line they have centred on.
Up-down what? This was my first question when reading this paper having never come across the approach before, so I’ll take a couple of lines and a dodgy drawing to try and explain it. This design uses the outcome of the patient before the current patient to determine what dose you will use. A success-fail binary outcome is predetermined (in this case the degree of motor blockade) and a predetermined starting dose is given to the first patient (in this case 7.5 mg of 0.75% plain bupivicaine). If the result is a success then the next patient gets a dose that has been reduced by a predetermined aliquot (0.75mg) and they see if this is a success or a fail. When a patient has a ‘fail’ outcome, the next patient gets their dose increased by the predetermined aliquot. This continues with the dose going up and down depending on the success or failure of the dose with the preceding patient. The result is an oscillation around the median effective dose that we are interested in. If there are 6 or more oscillations then we can be reasonably confident with the median line they have centred on.
The advantage they cite for this approach is that you don’t need many patients involved to get good degrees of confidence in your results. Indeed this study only had 129 patients divided across 6 cohorts, resulting in only 20, or just over, in each group. One disadvantage that is immediately apparent is that you are pushing the limits of the dose until you actually fail, which seems a rather unethical approach to subject patients too. The authors appear to have navigated this by using a combined epidural and spinal technique, allowing epidural top-ups in the event of inadequate spinal coverage.
What Did THey Find?
The results show a pretty convincing linear decline in dose requirement with increasing age. The median dose for the 71-80 group is a mere 5.78mg compared with the 10.22 mg in the 20-30 group, nearly half the dose! The incidence of side effects or the need for epidural top-ups was no different between the groups, as was the level of sensory block achieved.
Is It Any Good?
As a short answer, yes. The up-down sequential allocation technique is, as you may have guessed, not one I am familiar with. Based on what I’ve read about it though it seems a completely valid and indeed well suited approach to this sort of question (there are a few links at the bottom if you want to read a bit more about it). The rest of the study was well designed and conducted with careful standardisation of the other variables of the anaesthetic, blinding of the anaesthetists and fairly similar patient characteristics in the different cohorts, age being the clear exception.
One niggling point is the fact that the volume of injection also varied with the dose, meaning that the older cohorts got a significantly lower volume as well as total local anaesthetic dose. The authors noted at the start how these interlinked factors of dose, volume, concentration and baricity are all important factors in the effect of spinal anaesthetic, and the dose and volume have been changed simultaneously in this study, making unpicking the difference a challenge.
Finally, whilst the ED50 has greater accuracy in identifying the differences in drug potency, it doesn’t have immediate clinical applicability. Rather it is the ED95 or higher that we are wanting for our patients (a 50% chance of the anaesthetic working just isn’t good enough for some people...). As noted in some of the links on the up-down sequential allocation technique, problems with analysing this stem from the plateau nature of the dose response curve at higher levels, hence the use of the ED50 instead. It still tells us a great deal about the relative potency of bupivicaine as age increases, we just have to apply that knowledge clinically.
One niggling point is the fact that the volume of injection also varied with the dose, meaning that the older cohorts got a significantly lower volume as well as total local anaesthetic dose. The authors noted at the start how these interlinked factors of dose, volume, concentration and baricity are all important factors in the effect of spinal anaesthetic, and the dose and volume have been changed simultaneously in this study, making unpicking the difference a challenge.
Finally, whilst the ED50 has greater accuracy in identifying the differences in drug potency, it doesn’t have immediate clinical applicability. Rather it is the ED95 or higher that we are wanting for our patients (a 50% chance of the anaesthetic working just isn’t good enough for some people...). As noted in some of the links on the up-down sequential allocation technique, problems with analysing this stem from the plateau nature of the dose response curve at higher levels, hence the use of the ED50 instead. It still tells us a great deal about the relative potency of bupivicaine as age increases, we just have to apply that knowledge clinically.
Final Thoughts
Overall then this seems to be a well constructed study with pretty convincing evidence on the effect age has on decreasing the dose requirements for spinal anaesthetic. There didn't seem to be much in the way of significant risk of bias in the results, just questions about how to apply them to clinical practice. Low dose spinals are not something I have confidence in performing given the ‘one-shot’ nature of it but theoretically it seems sensible that the less we give, the fewer adverse effects we are likely to encounter. I’m not quite how this can be immediately translated into clinical practice, but this study suggests there is a fair bit of scope for reducing the doses we are giving to our older patients when comparing them to their younger counterparts. This isn't a study that changes clinical practice overnight, but I think it adds further evidence to the pile to help us make decisions on the spinal anaesthetics were are providing to our patients.
Thanks for reading and as always please let us know your thoughts.
Tom Heaton
Thanks for reading and as always please let us know your thoughts.
Tom Heaton
Links
Link to Paper - The discussed article from 'Anesthesia & Analgesia'
Explanation of up-down sequential allocation technique
NAP 3 - The 3rd RCOA National Audit Project looking at central nerve blocks
Link to Paper - The discussed article from 'Anesthesia & Analgesia'
Explanation of up-down sequential allocation technique
NAP 3 - The 3rd RCOA National Audit Project looking at central nerve blocks
Image courtesy of patrisyu/freedigitalphotos.net
 RSS Feed
RSS Feed
