
Last week I had the pleasure of attending the Group of Anaesthetists in Training Annual Scientific Meeting in Manchester (or GAT ASM for short). The two and a half day conference was packed with talks on everything from metacognition to haemorrhage management, and all supported by a healthy amount of tweeting (#GATASM15 if you fancy having a look back through all the chat). As with the previous conferences I’ve been on I came away with a whole raft of new exciting ideas, educational links, and great people to follow on Twitter. While I’ve no chance of covering all the great topics that came up, I’d hoped to put together a few notes on some of the most interesting and useful ones.
GAT ASM Homepage
GAT ASM Homepage
Feedback
The first day (though it only officially kicked off at lunchtime) had a number of top topics and speakers to get us warmed up. One of the speakers that stood out for me was Dr Neil Bacon, founder of none other than Doctors.org.uk, who was talking to us about his new and fascinating project; I want great care. As if creating ‘the UK’s largest network of doctors’ wasn’t enough, Neil wanted to create the Tripadvisor of the medical world, and provide a new way for patients to provide feedback to us. Patients can give their doctors a 5-star rating and add specific comments and feedback about what they thought was fantastic or poor. Great idea or horrible mistake? Well the start of his talk suggested that this had been a bit of a marmite topic, and indeed Neil’s opening gambit was to tackle the audience concerns head on. The audience answered his request to provide their concerns about this idea with a few important ideas; unrealistic patient expectations, reputational damage (that doctor killed my mum), trolling, and even slander by colleagues. All valid and understandable concerns which were duly answered by reassurance that, firstly, the site is well monitored with sophisticated software to detect many of these forms of abuse and apply a low threshold to intervene in cases of suspected falsification or campaigning. Secondly, Neil described how the vast majority of feedback was of a very positive nature and that the benefits clinicians described from receiving this were worth the exposure (‘It reminds me why I did this job’). Some of the concerns from an anaesthetist’s perspective put a slightly different slant on this, namely the degree of recall that can be expected of our role in their care – will it be primarily a bad experience that will be biased towards (analogous to expecting my pilot to fly smoothly and only recalling the flights that are particularly bumpy). However, Neil described his anecdote of his own serious injury that required 4 trips to theatre. One of those anaesthetics in particular stood out to him compared to the others with regards to how good he felt after it. Despite the jokes about anaesthetic technique that are applicable (‘that’s the anaesthetist that used dexamethasone’ was the one going round the audience) this is a point that really resonated with me. I don’t feel that our goal for our patient should be ‘yeah, but did you die?’ but rather that they experienced their surgery with the minimum amount of pain, nausea and general distress that we can manage and I’m pretty sure this is how the vast majority of us feel. I do think that this sort of feedback will become part of our revalidation process in the future and this seems to be a fantastic tool to show ourselves (and others) that we are providing great care.
iWantGreatCare
iWantGreatCare
Not the anaesthetist we want to be...
Fantastic talk from Neil Bacon on iWantGreatCare. Convinced me about the benefits of transparent feedback #GATASM15
— Thomas Heaton (@tomheaton88) June 17, 2015
Excellence
Yet barely had Neil sat down before Dr Adrian Plunkett was up on the stage with another great idea for our practice; excellence reporting. His opening observations clearly resonated strongly with the audience as he described how our system was very strongly focused on criticism, blame and negativity. The language of management had developed to reflect this with incident reporting becoming a verb (‘I’m going to IR1 you!’) and barely a clinical disagreement going by without a reference to clinical incidence reporting. His question was whether this was the best way to create a workforce that provided great care to patients? This seemed such an obvious truth and yet his description of the excellence reporting system he had introduced at his trust was an example of ‘why haven’t we thought of that?’. Many of the ideas echoed those that Neil Bacon talked about just previously in the sense that we seem to accept not receiving positive feedback as the norm. I do appreciate that our assessment processes have an increasing focus on demonstrating evidence of excellence, but it remains small and quiet compared to the components looking at ‘negative behaviour’. This isn’t to say that these aspects aren’t important, but that you don’t provide great care simply by targeting negative activity.
Changing incident reporting to excellence reporting. 'Root cause of awesomeness' #GATASM15
— Thomas Heaton (@tomheaton88) June 17, 2015
Earlier on that day there had been another top talk from Jim Corcoran, clinical director of peri-operative care at the fantastically performing Salford Royal Hospital. His talk on management was really fascinating for its insight into the problems with being a successful manager in today’s NHS. As he alluded to in his intro there is still an ‘us and them’ relationship between managers and doctors, that many clinicians feel that they would be ‘selling out’ if they went over to the dark side of management, and that such positions are inherently unstable posts (the average CEO’s term is 2 ½ years). This may explain why many of us still feel that barrier between our clinical work and that of management, which is unfortunate. I myself have particularly enjoyed the leadership and management talks I have attended, and Jim again highlighted the many benefits to having clinician engagement and indeed leadership in hospital and departmental management. Perhaps the key point was that you have to be engaged to push through the change that you want and that you see needs to happen from your time on the front line. His general point was that we should be aiming for excellence as an institution and aiming to deliver the very best service to our patients, and management is as vital to this as is doing our own personal job well. A few recommended reads that he made look very interesting and will certainly be crossing my path soon:
If Disney Ran Your Hospital – Fred Lee
Wilful Blindness – Margaret Heffernan
If Disney Ran Your Hospital – Fred Lee
Wilful Blindness – Margaret Heffernan
Metacognition
Adrian Plunkett was back the next day giving an introduction to metacognition. This is an area I already have a strong interest in and Adrian really demonstrated how important this ‘thinking about thinking’ is in our daily practice. He provided a quick run through of the basics of ‘Dual Process Theory’; the theory that we have a super quick, automatic, unconscious, and effortless way of thinking (System 1) and a slower, conscious, highly demanding mode (System 2). We use system 1 the majority of the time for obvious reasons (it’s easier) and, though it’s pretty good for most things, it is essentially just pattern recognition. As such it will lead to problems because of the complexity of medicine and life in general (Pattern: 20ml syringe of straw coloured fluid = thiopentone….or cefuroxime?). Basically, as clinicians we are in an environment where problems with our system 1 have a potential to cause significant harm, and probably even more so as anaesthetists. It would follow that a decent understanding of our natural biases and cognitive flaws is vital for minimising harm. The increased training in ‘human factors’ is a testament to this and a vital part of implementing all this ‘amateur psychology’ in something actually useful. That being said I do find reading about this topic fascinating and there are few books that were recommended on the topic that I have also found fascinating.
Thinking Fast & Slow: Daniel Kahneman
The Chimp Paradox: Steve Peters
Thinking Fast & Slow: Daniel Kahneman
The Chimp Paradox: Steve Peters
Earlier on the Thursday there had been a great talk on a similar topic by Tom Evans entitled ‘Performance: concepts from elite sport’. Tom is an ED physician who has worked, and still is working, with the Great British Olympic rowing team. His formula for success was a simple one:
Results = Knowledge x Skills x performance
The idea behind this is that performance is everything. Elite athletes get one shot at this medal every 4 years. They will have spent hours each day developing the knowledge and skills to the maximum, but unless they perform on the day they will lose. I think the analogy is perfect for highly demanding clinical specialities such as anaesthesia and critical care, the main difference being that we have no idea when we need to perform. I might need to perform an emergency surgical airway tomorrow, or never do one in my whole career, but I still need to perform pretty well to avoid disaster. I have put together the knowledge and skills for such an event (I’ll opt for scalpel rather than needle - NAP 4) but have I really optimised my performance for what is almost certainly going to be a horrendous situation? Will I act quickly, calmly and decisively when this can’t intubate, can’t oxygenate scenario presents itself? I am a big fan of simulation for this reason and really wished we had more chance to do this on a regular basis (weekly?) but Tom described how the world’s top, highest fidelity simulator remains the human mind. Top athletes visualise crossing that line in first place as a core part of their training. I think I will be spending a bit more time thinking about all the most horrific things that can go wrong, and how they shall be resolved in a calm and decisive manner. I don’t really want the real time to be the first time.
Results = Knowledge x Skills x performance
The idea behind this is that performance is everything. Elite athletes get one shot at this medal every 4 years. They will have spent hours each day developing the knowledge and skills to the maximum, but unless they perform on the day they will lose. I think the analogy is perfect for highly demanding clinical specialities such as anaesthesia and critical care, the main difference being that we have no idea when we need to perform. I might need to perform an emergency surgical airway tomorrow, or never do one in my whole career, but I still need to perform pretty well to avoid disaster. I have put together the knowledge and skills for such an event (I’ll opt for scalpel rather than needle - NAP 4) but have I really optimised my performance for what is almost certainly going to be a horrendous situation? Will I act quickly, calmly and decisively when this can’t intubate, can’t oxygenate scenario presents itself? I am a big fan of simulation for this reason and really wished we had more chance to do this on a regular basis (weekly?) but Tom described how the world’s top, highest fidelity simulator remains the human mind. Top athletes visualise crossing that line in first place as a core part of their training. I think I will be spending a bit more time thinking about all the most horrific things that can go wrong, and how they shall be resolved in a calm and decisive manner. I don’t really want the real time to be the first time.
Clinical
There was a bit of clinical content thrown in as well. Richard Griffiths opened the Thursday with a great talk about age anaesthesia. Even more interesting than his run through of the physiology of ageing was his analysis of the ‘epidemiology’ of it. It’s hardly news that we are facing an increasingly aging population but some of his visions were still a cause of concern given the financial and organisational challenges already faced by the NHS. Currently 77% of all acute inpatient episodes are patients aged over 65, but the baby boomer generation has still yet to reach that age. He predicted that some large centres will be operating on 6 hip fractures every day in the not too distant future; there may soon be specialised hip fracture anaesthetists. Despite this clear warning that we are all going to have to become specialists in age anaesthesia, he did keep some positive points for us. Namely that aging is not the sole culprit for the physiological deterioration that comes with age, but rather that there is a frequently an increasingly sedentary lifestyle with a number of detrimental results. The good news is that this is reversible we ‘prehabilitation’, and he described a few studies that show a meaningful benefit with exercise programs (listed at the end).
And Finally...
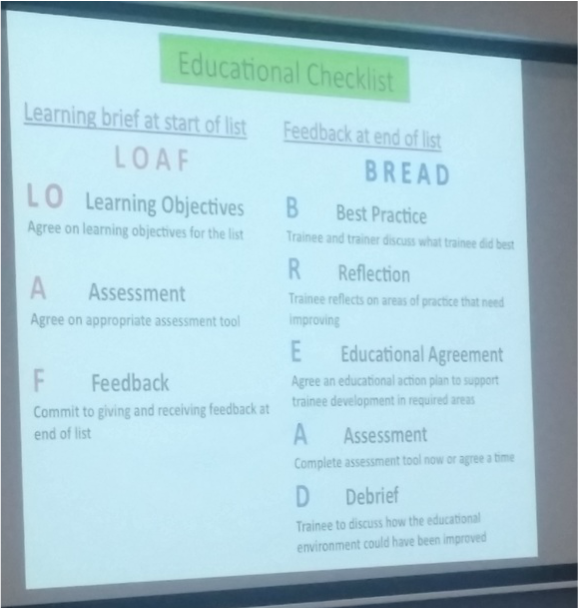
As I’m looking at the amount I have written so far it’s becoming clear that it’s time to wrap it up. Unfortunately I feel that haven’t covered many of the topics that were also very very good. There were a few really good sessions on education at GAT, with a great overview of adult learning theory by Cathy Armstrong. She also described a great little idea being driven in Manchester to optimise the learning opportunities from theatre lists (the acronyms being LOAF/BREAD). The conference also offered free mentoring sessions as a taster for what mentoring can offer us as trainees. After letting curiosity get the better of me I can say that is was well worth it, if not quite what I was expecting. There were some fascinating talks by a couple of our local trainees Matthew Jackson and Simon Forrington about their experience of working in an Ebola epidemic and as in aeromedical retrieval respectively. There were a number of great clinical talks that I haven’t got round to mentioning looking at major haemorrhage, peri-operative lung protection, aortic stenosis and ECMO amongst others. The ethics and law session was also a really interesting block, covering the challenging topics of consent, negligence claims and the use of social media (the Twitter feed went a little bit quiet during this session). The conference closed on a high with the very engaging debate about the future of anaesthetic rooms, the final vote going in favour of keeping them.
Major haemorrhage more common than CICO scenario but not as much focus on it in our training #GATASM15
— Thomas Heaton (@tomheaton88) June 17, 2015
Well thanks for making it this far. There was so much to talk about that it was a challenge to stop writing but I hope I have managed to cover a few interesting topics and provide some useful links to resources that were brought up during the 3 days. The twitter feed also has a wealth of top tweets with links and pictures that might be of interest (#gatasm15). I have to say a big thanks to the organisers for a great few days in which there wasn’t really an off note, as well as all the other great Twitter posters who kept a constant stream of interesting and engaging discussion going. As always please let me know your thoughts on any of the topics that have caught your eye or if you have other links that you have found interesting. Thanks again for reading.
Tom Heaton
Tom Heaton
Links
Excellence & Feedback
iWantGreatCare
If Disney Ran Your Hospital – Fred Lee
Wilful Blindness – Margaret Heffernan
Safety I & Safety II - Erik Hollnagel
Metacognition
Thinking Fast & Slow: Daniel Kahneman
The Chimp Paradox: Steve Peters
From Mindless to Mindful Practice
Clinical Cognition & Diagnostic Error
Clinical
Prevention of atelectasis
The PROPPR Trial
Skeletal Muscle Mitochondria Paper
CESAR Trial
Diastolic Dysfunction
Education
Adult Learning Theories
iWantGreatCare
If Disney Ran Your Hospital – Fred Lee
Wilful Blindness – Margaret Heffernan
Safety I & Safety II - Erik Hollnagel
Metacognition
Thinking Fast & Slow: Daniel Kahneman
The Chimp Paradox: Steve Peters
From Mindless to Mindful Practice
Clinical Cognition & Diagnostic Error
Clinical
Prevention of atelectasis
The PROPPR Trial
Skeletal Muscle Mitochondria Paper
CESAR Trial
Diastolic Dysfunction
Education
Adult Learning Theories
 RSS Feed
RSS Feed
