
Well for various reasons it has been a little while since our last post but we’re back with a review of a paper that was looked at during our more recent local journal club. The paper is entitled ‘Adequate antibiotic admission prior to ICU admission in patients with severe sepsis and septic shock reduces hospital mortality’ and is freely available via the link below, so definitely worth having a bit of a look at. Sepsis is probably the top condition we face in critical care, and indeed probably for hospital medicine as a whole. There have been big strides forward in the management of this massive killer, though we still seem a little way off understanding this very diverse condition completely. The triad of ARISE, PROMISE and PROCESS have expanded how we think about the resuscitation for the condition, but one of the lynchpins of treatment has always been early antibiotics. Indeed I think some of the numbers from Kumar et al.’s have been extrapolated to every infection through the widespread education of the Sepsis 6 (I don’t think my patient with a simple UTI will have a 7% increase in mortality from an hour delay in antibiotics, but the message is pretty widespread at least). So I was quite interested to see what this particular paper could provide in the way of improved understanding.
Adequate antibiotic admission prior to ICU admission in patients with severe sepsis and septic shock reduces hospital mortality
Adequate antibiotic admission prior to ICU admission in patients with severe sepsis and septic shock reduces hospital mortality
What did they do?
So the authors primarily set out to have a look at the effect of delayed appropriate antibiotics on mortality using a large database that they had put together over 5 years from a university hospital ICU. Using this database they looked at every patient admitted to the unit with sepsis and then looked for those with a subsequent microbiological isolate. This allowed them to assess whether the antibiotic they had received at whichever time was appropriate and would actually be effective – quite an important consideration. Using this cohort they were also able to apply a number of statistical tests to look at which of their recorded variables were associated with their interested outcome, in this case hospital mortality.
What did they find?
From an initial set of 926 patients, they selected a cohort of 638 (68.8%) who had a documented microbiological isolate (quite a good yield in my opinion). When they applied their statistical calculations to this cohort, looking at what impacted on hospital mortality, they found a few clear themes. The factors that were associated with a worse hospital mortality rate were:
A breakdown of the groups with different antibiotic timings provides a bit more information about what could be the important factors at play here. Of all the patients with a confirmed microbiological isolate the comparison shows that the group with a delay in receiving appropriate antibiotics until after ICU admission were more likely to have a hospital acquired infection and (probably related) a higher rate of ‘difficult to treat pathogens’. For me it is this breakdown that is probably most enlightening as to what this study is really showing, but there is a lot to be said about the causality etc. in such a study. However, it is interesting when it is noted that 98.3% of patients did receive some antibiotics before arriving on the ITU, suggesting that the delay wasn’t because nothing was given, rather that there were incidents when what they had wasn’t effective.
The other finding were rather less revolutionary, demonstrating that if you had features of a worse baseline (e.g. Cirrhosis, malignancy, immunosuppression) or severity of illness (septic shock, APACHE II score) then you were also more likely to day. There is probably a reason why they didn’t make the headline of the paper, but it always useful information to have.
- Delay in ‘appropriate’ antibiotics until after ICU admission (the headline of the paper)
- Acutely sicker patients – Septic shock, higher APACHE II and SOFA scores.
- Chronically sicker patients – immunosuppression, cirrhosis, malignancy, age
A breakdown of the groups with different antibiotic timings provides a bit more information about what could be the important factors at play here. Of all the patients with a confirmed microbiological isolate the comparison shows that the group with a delay in receiving appropriate antibiotics until after ICU admission were more likely to have a hospital acquired infection and (probably related) a higher rate of ‘difficult to treat pathogens’. For me it is this breakdown that is probably most enlightening as to what this study is really showing, but there is a lot to be said about the causality etc. in such a study. However, it is interesting when it is noted that 98.3% of patients did receive some antibiotics before arriving on the ITU, suggesting that the delay wasn’t because nothing was given, rather that there were incidents when what they had wasn’t effective.
The other finding were rather less revolutionary, demonstrating that if you had features of a worse baseline (e.g. Cirrhosis, malignancy, immunosuppression) or severity of illness (septic shock, APACHE II score) then you were also more likely to day. There is probably a reason why they didn’t make the headline of the paper, but it always useful information to have.
Is it any good?
I myself was rather in two minds about this question. My first reaction is that this isn’t a particularly good study from a methodological perspective. Part of the journal club discussion was how there isn’t really any way to feasibly conduct a high quality study on such a topic because of the powerful evidence of the benefits of early antibiotics (randomising people to placebo antibiotics isn’t going to go down well with the ethics board). However, there was some suggestion that the premise of the study was actually a result of some data ‘fishing’ by the authors with their nice big patient database, rather than a prospective cohort study looking at an initial focused clinical question. They’ve done the usual statistical analysis to try and demonstrate that the two cohorts are otherwise pretty similar to each other and therefore these results are meaningful, but there still seems to me a relatively high risk of confounding factors with this methodology. I’m also a bit unsure about the use of ICU admission time as the criteria of choice for differentiating between the two groups. Again the concern with this is that it’s just where the numbers looked best rather than following a particular clinical enquiry that was determined prior to data collection. It might be that this wasn’t the case, but the description of their methodology is pretty ambiguous around this point.
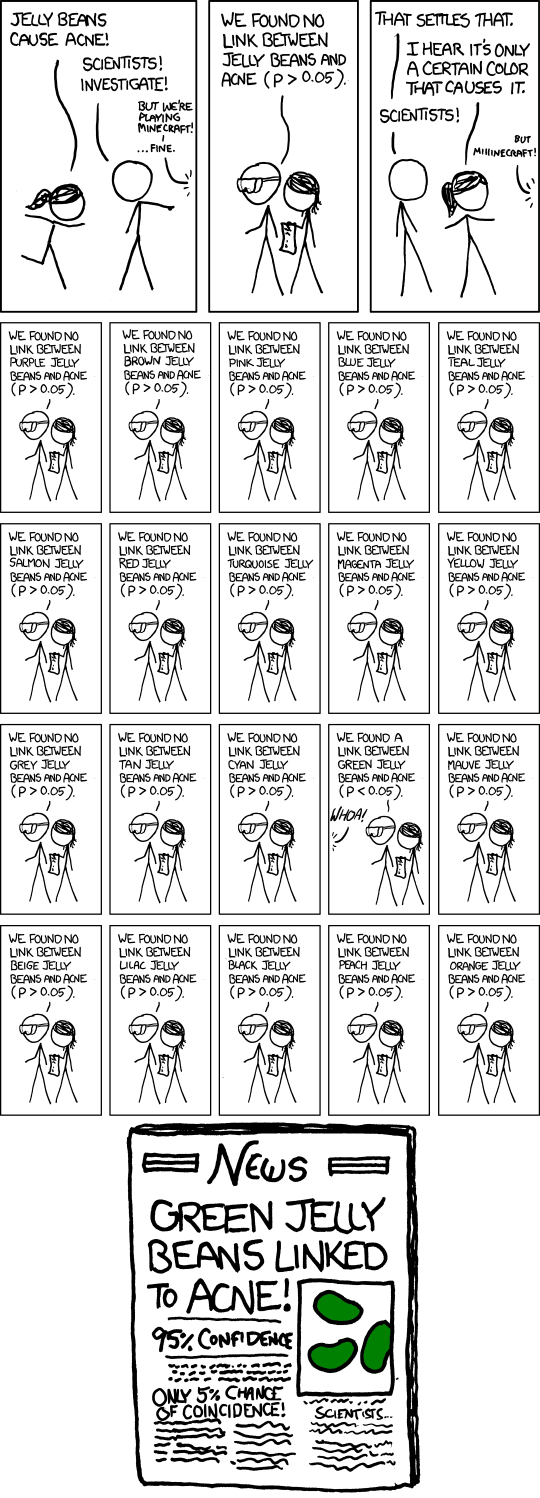
All this being said, the results demonstrated are fairly powerful and suggestive of sensible mechanism of actions in some regards. An absolute difference in hospital mortality of 20% is not trivial, and there would need to be some significant bias and confounding present to question such a result, especially as the number of patients is fairly decent. This is similar for a few of the other results that have cropped up with their multivariate analysis, such as the difference in ‘difficult to treat pathogens’, and they paint a rather nice picture of causality. There are certainly dangers in this approach to stats though (I think the cartoon from the excellent XKCD demonstrates it brilliantly).
All this being said, the results demonstrated are fairly powerful and suggestive of sensible mechanism of actions in some regards. An absolute difference in hospital mortality of 20% is not trivial, and there would need to be some significant bias and confounding present to question such a result, especially as the number of patients is fairly decent. This is similar for a few of the other results that have cropped up with their multivariate analysis, such as the difference in ‘difficult to treat pathogens’, and they paint a rather nice picture of causality. There are certainly dangers in this approach to stats though (I think the cartoon from the excellent XKCD demonstrates it brilliantly).
Final Thoughts
Overall, I think I would have to say that there are some important messages that can be drawn from this paper, as long as there is some caution in this interpretation because of the way they have been gathered. It seems to repeat what previous studies have shown us; a delay in antibiotic administration in sepsis worsens mortality. Importantly for practicing clinicians, this antibiotic has to be something that the offending pathogen is sensitive to. Now this would seem obvious, but there is definitely an increasing problem with resistant pathogens in critical care medicine. Often the urge is to give antibiotics ASAP, perhaps preventing a careful trawl through previous culture samples and chasing a microbiology opinion, not to mention the challenges in narrowing down a likely source in a condition as variable in its presentation as sepsis. Yet this decision could be one of the most important decisions we make in terms of a patients outcome, particularly if this a patient with a significant healthcare history where the chances of a resistant pathogens is high. I do slightly feel that this is therefore more relevant to the construction of local antibiotic policies than to the clinicians following them, but an appropriate policy won’t be of use without a careful think about the relevant clinical features.
So in summary:
Tom Heaton
So in summary:
- A delay in appropriate antibiotics increases hospital mortality
- There is probably an increased risk of this with difficult to treat pathogens (probably due to resistance to initial treatment) and this may be linked to the association with hospital acquired infections.
- Think carefully about what organisms you are treating when you reach for the antibiotics – that choice may significantly affect the patient’s chance of survival.
Tom Heaton
References
- Garnacho-Montero, J et al. Adequate antibiotic admission prior to ICU admission in patients with severe sepsis and septic shock reduces hospital mortality. Crit Care. 2015. 19(1): 302
- Kumar, A et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006. 34: 15989-1596
Lower mage courtesy of XKCD.com
p.s. I would like to add my thanks to everyone that took part in our local journal club who made several contributions to the discussion that has led to this post.
 RSS Feed
RSS Feed
